There is a 55-year-old woman who has lived in northern Iraq for most of her life. In 1974, she married a farmer and by 1988 had six children with him—four girls and two boys. She lived in close proximity to her family—three sisters and two brothers who, together with their husbands and wives, had more than 50 children among them. It was also in 1988 that Saddam Hussein sent soldiers to her village, separated the men from the women and children—including 68 members of her family—and transported them to a place called Noogra Salman in central Iraq. In less than one year’s time—exactly 236 days—she watched 20 members of her family die slow deaths due to malnutrition, mistreatment, lack of sanitary living conditions, and other abuses.
Today, this woman, one of her daughters, and two of her nieces are the only family members of the original 68 known to have survived. Her life forever marred through her suffering from the long-term effects of post-traumatic stress disorder (PSTD) and depression, she recently made her way to the trauma recovery and training center in Sulaimania, where she is now receiving treatment. It’s a miracle of sorts in a country where mental illness is looked down upon and mental health workers are shunned in the Middle East. In Iraq, even those who are trained to give treatment to those suffering from mental illness carry this stigma.
(For reasons of security, I cannot share with you her name or other identifying details—or that of any other “survivors” mentioned in this article. Out of respect, I have chosen not to give these survivors pseudonyms—I leave it up to you to provide them with names.)
Located on a corner property facing a small but heavily transited road, the brand new facility—a previously unused building provided by the Kurdistan Ministry of Health and rehabilitated with $30,000 from the USAID Provincial Reconstruction Team and run under the auspices of the international arm of Heartland Alliance for Human Needs and Human Rights, a non governmental organization, or NGO, based in Chicago—had its formal opening on July 8. The center has been in operation since early January, with staff working out of a much smaller building. After three years, the building will revert back to the Ministry of Health, which according to its medical director, Dr. Ahmed Amin, is a good thing. “Government involvement adds to our potential sustainability,” he says. “Once the NGOs cut their funding, more than likely, the government will continue to fund the center.”
Since its opening, the center has seen approximately 60 clients. Dr. Amin explains that the site is a training facility as well as a treatment center providing three kinds of service: “medical, psychiatric, and psychosocial. Basically, we do training and treatment. We treat individuals and groups such as families. And we also have a training component where we have conducted trainings for social researchers, psychologists, medical staff.”
DESIGN, MONITOR, AND EVALUATE
The center is a work in progress, with training procedures and treatment techniques under strict evaluation and review under the guidance of Heartland Alliance, experts from their Marjorie Kovler Center for the Treatment of Survivors of Torture and from Johns Hopkins University. “Our role is to assist NGOs in designing, monitoring, and evaluating mental health programs around the world,” says Paul Bolton, an associate scientist at the Center for Refugee and Disaster Response of the Johns Hopkins Bloomberg School of Public Health. Bolton has been working since 1988 both with victims directly and as a technical consultant with NGOs in war, disaster, and development settings, including Rwanda, Cambodia, Angola, Mexico, and Kazakhstan. The Victims of Torture Fund at USAID partially funds Bolton’s work and it was USAID that asked him to work with Heartland Alliance and its trauma recovery and training center in Sulaimania.
“You can’t have any design without data, so we do a process of needs assessment, says Bolton. “So, for example, for torture survivors here in Sulaimania we assist in designing programs by first assisting in collecting data.” Bolton began collecting data last April interviewing 70 torture survivors around Sulaimania using ethnographic interviewing methods. The questioning was open-ended. Yes/no, multiple choice, and leading questions were avoided. Trained interviewers spoke with the torture survivors on two separate occasions, probing them to give as many answers as possible to specific questions. Interviewers were also trained to set up a rapport with those they were interviewing.
“If you show interest, and you’re not judgmental, you find that people just start to open up,” explains Bolton. “And then if you go back a second time and interview them again, you find that the second interview is usually much better than the first. We find in limited interviewing that if you ask a person, ‘What are your problems?’ they’ll just rattle off five or six to the last person who asked them or repeat what everyone else is saying. But if you ask somebody an open-ended question you’ll find that after the first five or six answers ,they actually start to think. And it’s the ones you get after the first five or six that are valuable.”
Ethnographic studies are usually very small but produce in-depth responses that allow researchers to better gauge what the salient issues are. Since most NGOs like Heartland Alliance have limited capacity and are unable to deal with all the issues, Bolton’s process has helped them to formulate which issues are not only most important, but most addressable. “We always get more problems than we can address, so Heartland Alliance has to choose. In this case, it’s a mental health program, so which mental health problems you can actually deal with is determined by this process.”
For the most part, Bolton’s research revealed the usual mental health problems of depression and anxiety normally associated with traumatic experiences. But there were some surprises. “In other countries, when you have people who have been tortured for something like a cause—like people who were tortured by Saddam, people who went through the Anfal from Saddam, or people who fought for the Kurdish forces—what we usually find is that those people would be respectable after the event,” he says. “What has happened here in Kurdistan is the opposite. People have said to us, ‘You know, we are the bottom of society. The people who did not fight, who did not suffer do not respect us. In fact, they look down on us as fools saying why did you suffer? You are a fool.’ Even our families say this.”
According to Bolton, the particular feeling of inferiority felt by survivors adds to their mental health problems. In all his years of research and work in this area, he has never come across this scenario. “[With] people who have suffered for some kind of cause,” he explains, “at the very least the people around them say this was a good thing and they feel some respect even if they don’t feel mentally well.”
The other issue Bolton’s research revealed was a sense of betrayal at the hands of the Kurdish government. “This was amazing,” he recalls. “Almost to a man and a woman, the interviewees said, ‘This Kurdish government has betrayed us. We feel betrayed. We, too, feel that we were foolish to fight for this government.’”
An example of how some feel betrayed was vividly expressed in March 2006 in what Iraqi journalist Mariwan Hama-Saeed, a resident of Halabja, reportedly called a “spontaneous act of rage” that saw thousands riot and torch the controversial Monument of Halabja Martyr, burning it to the ground on the annual day of commemoration organized by Kurdish political leaders. The modern, 100-foot-tall memorial was supposedly built to honor the reported 5,000 killed and 10,000 injured as a result of poisonous gasses dropped by Iraqi planes in what is considered the largest-scale chemical weapons attack directed against a civilian-populated area in history. However, located on the outskirts of Halabja, far from the rubble of the true site of the attack, townsfolk claim the memorial was simply built for use as a staging ground for corrupt politicians to capitalize on the attention, international visitors. “Every year, officials come and they promise to rebuild the town and to take care of the sick people,” Hama-Saeed reportedly said, “but they never keep their promises.” As reported by Slate in June of 2007, “The village has been particularly hard-hit by government corruption and is in desperate need of this money. The town’s residents—most of whom must pursue costly treatments to deal with the residual affects of the attack—navigate unpaved roads strewn with trash, have spotty access to water and electricity, and live in ramshackle hovels made of concrete and scrap metal.”
WHO GETS TREATED
The people being treated at the center can be divided into three groups, explains Dr. Afram Hassan, an Iraqi psychiatrist—he is one of three in all of the governorate of Sulaimania with its population of 1.7 million people. “First, there are the people who have been tortured by any source, either by an authority or some other group, for example, at the hands of a political group,” he says. “This group also includes those who are suffering from depression due to the witnessing of trauma, such as bombing and other events of war. The second group contains cases related to the Anfal genocide. We have many people, who in 1988 by way of a special project of the previous government of Iraq—the Baath regime—destroyed approximately 5,000 villages and removed 182,000 people and forced them to relocate to the mid and south of Iraq. Some of these people escaped later on and returned back to Kurdistan. But most died in the places where they were relocated.”
The third group of people that visits the center seeking help are victims of gender-based violence (GBV), a widespread problem in the region. Since the trauma center has been open, Dr. Hassan has only seen 10 cases related to GBV. Although it is a small figure, Dr. Hassan cautions that one should not be mislead. “If you take into regard what we see in Sulaymania’s mental health center and hospital, and what we see our clinic here, everyday we are faced with this problem,” he says. “Despite all the attention given to it by the media and major organizations, cases of GBV remains a growing problem in the region with most occurrences happening in the villages rather than the city.”
The number of victims of GBV is actually so large that Dr. Hassan says, “If we opened our center directly to deal with this problem we would need a larger staff. Even if we multiplied our staff by 10, we could not deal with this problem. So we just deal with a limited number cases.” With several centers in Sulaimania and one in Irbil dealing specifically with issues of GBV, the center usually recommends them to GVB victims as the more appropriate place to go for treatment. However, some refuse to go to these other centers that specialize in GBV, “and so we deal with them,” says Dr. Hassan. “But we try to concentrate on Anfal and torture victims.”
THE “PATIENT” GROUP
There is a 44-year-old man who has lived most of his life in northern Kurdistan. Imprisoned from 1982 to 1986, he received different types of torture both physically and psychologically. Information on where or by whom he was imprisoned is not available, but a record of his experiences is. Prevented from eating or drinking for more than one week, he would only be allowed to take a small bit of food each day, but never any fruit or vegetables. He was never allowed any form of communication such as visits or letters from family or friends and he received electrical shocks to his tongue, head, and testicles on a frequent basis. Deprived of sleep for periods of six days, on some occasions he was suspended by his feet with his hands tied behind his back for periods of eight hours, and on others prevented from going to the bathroom for four-day periods due to the placement of a “tight thing” in his rectal canal.
The Trauma Recovery and Training Center is unique in that it in one of a small number that treat an ever-expanding number of torture victims and survivors. Although torture has been getting an ever-increasing amount of attention due to the work of international organizations such as the Red Cross, Human Rights Watch, and Amnesty International; media coverage of abuses at places like Abu Graib and Guantánamo Bay; and the actions of a Bush administration that appears to be bent on legalizing torture under its War on Terror doctrine, efforts to treat victims of torture are minimal. According to Sune Segal, spokesperson for the International Rehabilitation Council for Torture Victims (IRCT), there are only 200 to 300 such centers worldwide. “I cannot give you an exact figure of specialized centers and programs for torture victims worldwide,” says Segal. “What I can tell you is that the IRCT comprises a membership of some 140 such centers and programs in 70 countries. It is a question of definition; there are numerous clinics and programs that treat torture victims without this patient group being their primary target.”
While there is no good epidemiological information on the exact numbers of victims of torture or its survivors in Kurdistan, according to Heartland Alliance’s Scott Portman, “The number is in the hundreds of thousands, both before and subsequent to the fall of the regime.” The center has eight staff people, seven of them in clinical roles: one psychiatrist, one physician, and one psychologist, two senior mental health workers and two case managers. Victims of torture who have been seen by center staff date their experiences relating to periods of incarceration as far back as 1980. “We don’t pay attention to the time the person was put in prison or what specific kind of torture they have experienced,” says Dr. Hassan, who also sees clients at other mental health facilities in Iraq. “But we deal with the recent situation of this person: What are his mental or physical problems?” He explains that the details of where the person was tortured, how, and by whom are not ignored, but recorded, stored in the client’s file and added to the center’s database. But it is their treatment and care that are the focus.
When asked if he has treated any people who had been at Abu Graib, he says, “Yes. From Abu Graib, from Baghdad, from Kirkuk and from many areas. However, most of the cases [stem from] Anfal.” But there are also more recent cases. “For example, I have a case of a person who was kidnapped in Baghdad for about 10 or 20 days and released after a payment was made of $100,000. This person received a large amount of torture,” he recalls. “As you know, $100,000 is not an easy amount to come up with.” Dr. Afram said the man claims he was taken by the US military while he was at work, at some point later on was handed over to an Iraqi group in a different area not in control of the US military, and was finally released after the payment was made.
“The US military released him?” I ask.
“No, not exactly released,” says Dr. Hassan. The man claimed he was handed over to the second group, who phoned his wife and told her she should pay $100,000 in exchange for her husband. “This is a very tragic event. Until now, this person continually mentions and has flashbacks of what happened. He still asks, ‘I cannot understand why the US Army [took] me and then later on gave me to this group [who demanded the money].’ Until now, he says, ‘I am sure the US Army soldiers take some of the amount of this money from this group. For this reason they give me to this group.’” Working in Baghdad since 2003, Dr. Hassan says that five or six of his clients have claimed that the US army is engaged in this kidnapping activity in the middle of Iraq. (Due to client-patient confidentiality strictures, the stories of Dr. Hassan’s patients being abducted by groups in collusion with members of the US Army could not be verified.)
“But also, as you know, these groups in the middle and south of Iraq are very active,” he adds. “All say they are from a Sunni or Shiite group, and take a person from this group and later on replace it to the other.” Convinced it is done purely for business purposes, he explains, “For example, a Sunni group will take 30 to 40 persons of a Shiite group. And later on, this Shiite group will take some amount of the Sunni group. Later on, either they release them in an exchange with each other, or they take money from each other.”
ANFAL
One Barzani woman described the roundup of the menfolk: “Before dawn, as people were getting dressed and ready to go to work, all the soldiers charged through the camp [Qushtapa]. They captured the men walking on the street and even took an old man who was mentally deranged and was usually left tied up. They took the preacher who went to the mosque to call for prayers. They were breaking down doors and entering the houses searching for our men. They looked inside the chicken coops, water tanks, refrigerators, everywhere, and took all the men over the age of 13.
In his PBS “Frontline” report The Crimes of Saddam Hussein: 1988, The Anfal Campaign, Dave Johns says, “Al–Anfal, which is Arabic for ‘the spoils of war,’ is the name of the eighth sura, or chapter, of the Koran. It tells a tale in which followers of Mohammed pillage the lands of nonbelievers. Some say the government chose the term for its campaign against the Kurds of northern Iraq because it suggested a religious justification for its actions. Saddam’s Anfal was a mammoth campaign of civic annihilation, displacement, and mass killing.”
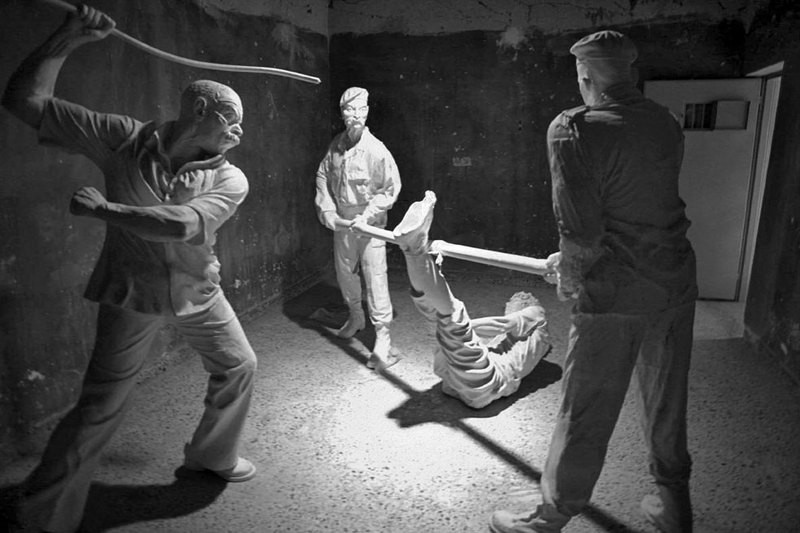
For over two years, from March 29, 1987, to April 23, 1989, a genocide and gendercide campaign was orchestrated by Ali Hassan al-Majid, better known as “Chemical Ali,” under the special powers granted him by his cousin, Saddam Hussein. Although reported numbers differ, it is widely believed that up to 180,000 Kurdish men, women, and children were exterminated and 5,000 of their villages were destroyed. According to an extensive report written by Human Rights Watch, tactics of the miniature holocaust that consisted of eight separate attacks included the widespread use of chemical weapons in addition to “mass summary executions and mass disappearance of many tens of thousands of non combatants, including large numbers of women and children, and sometimes the entire population of villages” and their infrastructure “including all schools, mosques, wells, and other non residential structures in the targeted villages, and a number of electricity substations.” Hundreds of thousands that were not disappeared underwent forced displacement—“trucked into areas of Kurdistan far from their homes and dumped there by the army with only minimal governmental compensation or none at all for their destroyed property, or any provision for relief, housing, clothing, or food, and forbidden to return to their villages of origin on pain of death.”
During this campaign, as decreed by al-Majid, all males found in the “prohibited areas” (despite the fact that these were their own homes and lands) were to be “detained and interrogated by the security services and those between the ages of 15 and 70 shall be executed after any useful information has been obtained from them.” As captured Kurdish populations arrived at detention centers, in Nazi-like fashion men were separated from women and small children, registered, warehoused under conditions of horrible overcrowding and deprivation, beaten, and after a few days taken out and trucked to sites where they were executed. In many cases women, children, and the elderly were also executed.” Those not exterminated were shipped to overstuffed relocation camps, where they were allowed to die of extreme malnutrition and disease.
Some groups of prisoners were lined up, shot from the front, and dragged into pre-dug mass graves; others were made to lie down in pairs, sardine-style, next to mounds of fresh corpses, before being killed; still others were tied together, made to stand on the lip of the pit, and shot in the back so that they would fall forward into it—a method that was presumably more efficient from the point of view of the killers. Bulldozers then pushed earth or sand loosely over the heaps of corpses. Some of the gravesites contained dozens of separate pits and obviously contained the bodies of thousands of victims.
A handful of the survivors, mostly women, have made their way to Sulamania’s Trauma Recovery and Training Center. “For most of these women, the man will not return back because he has been killed by the previous regime,” says Dr. Hassan. “Today, we have many widows, maybe 15,000 women, who, ’til now, don’t know where their husband is. Just the females returned back. Most of these women are not present in Sulaimania, but are present in areas south of Kurdistan—Kalar, Kifree, Khanaqan in the Diyala province, and Kirkuk.”
One patient, a 40-year-old woman, along with her five children, was purposely separated from her husband and forced to relocate as part of the Anfal campaign. Due to lack of food, lack of proper hygienic facilities—“lack of everything,” Dr. Hassan says—“two of her children died before her very eyes.” In this woman’s case, there was no place to bury her dead children. With nowhere to go, she was forced to watch as animals devoured their bodies. According to Dr. Hassan, this story is not unique. “We have many many tragic stories just like this here in Sulaimania. I’ve had between 10 and 20 cases that mention this sort of tragedy.”
WHAT WOULD FREUD SAY?
“I am always very surprised by the need for clear signs to realize that the person is dead. Freud talks of the test of reality. When someone dies, the first reaction is denial, then the external signs arrive from the outside confirming that this is what happened. That’s strongly reinforced in cases where people were not able to see. They heard the screams. It’s so desperate. The image of being on the other side of the hill. hearing the screams and the machine guns. You get stuck on that image and can’t go beyond it. You need to see the body.”
Once the problems illuminated by Paul Bolton’s ethnographic research study are identified and decisions are made by Heartland Alliance as to which they are capable of addressing, the work of discerning treatment begins. Who gets what treatment? On the road to answering this question, Bolton has created a long questionnaire of approximately 100 questions. With the help of some of the approximately 240 medical staff members that Heartland Alliance has trained as community mental health workers that currently operate in 15 out of Iraq’s 18 governorates, Bolton plans to use the questionnaire to interview another similar but different set of torture survivors to get feedback on the questionnaire itself. A revamping of the questionnaire will then take place and the final product will be used to screen torture survivors.
“We’ll screen people for the problems, give them the intervention, and then after the intervention we’ll re-interview them and see if they got better,” he says. “Do some types of people get better and other types of people not get better? Do they get better in some ways and not in other ways? Is it a good intervention? Yes, let’s expand it. Is it a bad intervention that did nothing? Let’s get rid of it. This is actually rarely rarely done, particularly in international settings. You’ll find huge libraries full of books talking about all the interventions you can do with people, but if you went to the literature you’d find there is no evidence that they work.”
Given that Bolton’s research has revealed this never-before-seen lack of respect given torture victims, which in turn spawns tremendous feelings of inferiority and only adds to the patient’s mental illness, will some innovative intervention need to be created? “Well, it’s going to require at least an adaptation from what we normally do,” he maintains. “We are going to have to think this through. Also, my recommendation to Heartland Alliance is, they will need to do more than just a mental health intervention. They need to talk to the government about how they treat these people.”
High hopes indeed in a country that regards mental health work as abnormal. “Here in Sulai, we only have three psychiatrists,” say Dr. Hassan, who received his PhD from Baghdad University. “In another few months another two doctors will graduate and come here and we will become five psychiatrists, if these two students graduate. The population of Sulaimania is about 1.7 million.” Not only is there a dearth of psychiatrists in Iraq—there are about 50 in the country, with less than 15 of them in Kurdistan—but for those brave enough to choose the profession, life is difficult. According to Dr. Hassan, a family practitioner or a dermatologist can see between 70 and 100 patients per day, psychiatrists can only see eight to 10 “because each one needs about 20 to 30 minutes. The dermatologist fee is the same as mine—10 dinars, or $8 per patient.” Thus, psychiatry is regarded as the poor branch of medicine. “It is difficult for you to build a house or buy a car, even difficult for you to marry,” he says. Marry? “Yes, because not every person will accept you as a man. Most people, especially prospective brides, regard you as abnormal,” he explains. “A psychiatrist is regarded as a stigma.
Not just the disease, but any person working in this field of mental illness, which is regarded as a stigma, is also regarded as a stigma. So not every woman will accept marriage to a psychiatrist.”
Not daunted by such realities, Dr. Ahmed Amin, the center’s medical director, has high hopes of his own. “Our goal is to be included in the curriculum of the University of Sulaimania,” he says. “That the university will send their students to the hospital and this clinic to get special trainings and participate in internships. We’ve [discussed] this with the vice-president of the University of Sulaimania and he was pleased with the idea. And also, hopefully, this year we will approach their college of medicine and college of sociology.”
When I ask how many victims of torture are in Iraq, Dr. Amin chuckles nervously. “How many victims of torture are there? So many, so many.”
“Millions? Thousands? Hundreds of thousands?” I ask.
“Maybe. Or millions.”
“So it’s an impossible job,” I say.
“Difficult but not impossible. We have started this center. It is in a small building, as you can see. We have a small number of staff. In all the world there are 200 programs and centers for torture survivors. I know 145 ratified the anti-torture convention, but so many countries participate in torture. So if you compare this center to all the need of Iraq…”
It is a finger in the dike.
“Exactly. But still, there should be a point where we should begin.”